Most people evaluating a weight-loss injection ask the obvious questions first. Does it work. What does it cost. What will it do to my stomach in the first few weeks. Those are reasonable places to start, but with an injectable medication there is a question that sits upstream of all of them, and it gets asked far less often than it should: where did this vial actually come from, and under what quality standard was it prepared? For a drug that goes under the skin rather than through a pill bottle, that question determines whether the contents match the label at all. Everything else follows from the answer.
This piece is organized around that upstream question. It sets out the routes by which liraglutide can legitimately be obtained, the route that should be avoided outright, and a short checklist a patient can apply before any purchase is made. It is written for orientation, not for making anyone’s individual treatment decision, and it stays close to what the underlying evidence and FDA record actually say.
One scope note before anything else. Liraglutide is a prescription medicine. The branded products carry FDA approval; compounded versions of the same molecule are a related but distinct product that does not carry that approval. Whether liraglutide is the right drug for a given person is a clinical judgment that belongs to a licensed prescriber who knows that person’s history. This guide is about sourcing and pharmacy standards, nothing more.
Why the source matters as much as the science
Liraglutide is a GLP-1 receptor agonist, and its FDA approval is genuine and long-standing. The weight-management version is sold as Saxenda, taken once daily and titrated up to 3 mg; the same molecule at lower doses is marketed as Victoza for type 2 diabetes [1][2]. The efficacy data behind it are solid and specific. In the SCALE Obesity and Prediabetes trial, adults without diabetes lost a mean of approximately 7.9% of body weight at 56 weeks on liraglutide, against approximately 2.6% on placebo. In the SCALE Diabetes trial, adults with type 2 diabetes lost approximately 6.0%, against approximately 2.0% on placebo [3][4].
Those numbers, however, describe a properly manufactured drug administered under supervision. A trial result belongs to the actual product that was studied, not to a powder of uncertain origin sold under a research label. That is the entire reason pharmacy quality deserves top billing here: dosing accuracy, side-effect management, everything downstream, assumes the product in the vial is what it claims to be. If the sourcing is wrong, the trial data simply stop applying, because the patient is no longer taking the drug those trials tested.
There is also a specific safety profile attached to liraglutide that makes the dispensing context more than a formality. The FDA label carries a boxed warning about thyroid C-cell tumors seen in rodent studies and a contraindication for anyone with a personal or family history of medullary thyroid carcinoma or MEN 2 [1]. The dose is raised gradually over several weeks specifically to manage the nausea, vomiting, and diarrhea that tend to cluster around escalation [1]. None of this argues against the drug. It argues for taking seriously who is dispensing it, who is prescribing it, and how closely someone is watching the process.
Here is the reframe worth sitting with. Liraglutide occupies an unusual position in the GLP-1 story right now: old enough to carry a decade of real-world and trial safety data, including the strongest cardiovascular outcomes data in its drug class, yet visibly outpaced on weight loss by the newer weekly agonists that followed it. That combination, a known quantity that is no longer the most powerful option, creates a particular temptation: shop for it on price, since it is “just” liraglutide, and the branded product isn’t cheap. That temptation is exactly what pushes some buyers toward the unregulated corners of the internet, and it is exactly why the sourcing question deserves more scrutiny for this drug, not less.
The three routes that meet the standard
Three paths for obtaining liraglutide hold up to scrutiny. Each looks slightly different in practice, but all three share the same backbone: a licensed pharmacy is involved in preparing or dispensing the product, and a clinician stands behind an actual prescription.
Branded medication through a licensed pharmacy. Saxenda or Victoza, manufactured by the originator and filled by a licensed retail or mail-order pharmacy against a valid prescription, is the cleanest of the three. This is the exact product studied in the trials cited above. Its identity and quality are not an open question. For anyone who can access branded product, this route carries the least ambiguity by a wide margin.
Compounded liraglutide through a licensed compounding pharmacy. Compounding pharmacies prepare medications to order, under state and federal oversight, and compounded liraglutide dispensed this way against a valid prescription is a legitimate option, so long as one fact is stated plainly rather than left implied: compounded liraglutide is not FDA-approved and is not the identical product as the branded pen. A pharmacy or provider operating in good faith says this outright. Within that honesty, a licensed compounding pharmacy working to recognized quality standards is a credible source.
Telehealth that routes through licensed pharmacies. Telehealth services that pair a real clinical evaluation with fulfillment through licensed pharmacies, branded or compounding, combine the first two routes with remote convenience. Whether this route is trustworthy comes down entirely to two facts: is the clinical evaluation genuine, and is the pharmacy genuinely licensed. Where both hold, this is a sound way to get the medication, and for most people shopping online today, it is the route that actually applies to them.
The thread connecting all three is accountability. A licensed pharmacy answers to regulators for what leaves its shelves. That accountability, more than any single ingredient test, is what keeps the vial’s contents tethered to its label.
The one route that fails, categorically
There is a fourth route, and it does not sit on a spectrum with the other three. It fails outright.
“Research use only” sellers. A meaningful share of the “liraglutide” sold online arrives as a vial or powder marked “for research use only” or “not for human consumption,” with no prescription and no clinician anywhere in the transaction. That label is not a bureaucratic footnote. It is the exact mechanism by which the seller steps outside pharmacy oversight and disclaims any responsibility for what happens when a human injects the contents. Nobody accountable has verified the product’s identity, its purity, or whether the labeled dose bears any relation to the actual one.
The case against this route is stronger for liraglutide than it would be for a drug with no approved alternative. There is no dilemma here between an unregulated product and no product at all. An FDA-approved version exists, and a supervised compounded version through a licensed pharmacy exists too [2]. Choosing the research-use-only route, then, isn’t a workaround for scarcity, it is a trade: give up verified product identity and clinical oversight in exchange for a lower price on something whose quality nobody can confirm. Measured against pharmacy standards, that trade does not clear the bar.
Five checks a patient can run before buying anything
None of these require special expertise. All of them can be checked before money changes hands.
1. Is there a real prescription behind it? A legitimate source requires an actual clinician evaluation and a prescription. If the product can be purchased with no clinician in the loop at all, this is disqualifying on its own, and for an injectable that requires careful titration, it is the single most important check on this list.
2. Is the dispensing pharmacy licensed and named? Legitimate providers can tell you, plainly, which licensed pharmacy fills the prescription. Evasiveness on this point is itself a red flag; licensed pharmacies are used to being named, because they are used to being regulated.
3. Does the label say “research use only” or “not for human consumption”? That phrase alone is enough to rule a source out. It tells you the product sits outside pharmacy oversight and that the seller has explicitly declined responsibility for human use.
4. Is the approved-versus-compounded line drawn clearly? A trustworthy source says, without hedging, that branded liraglutide is FDA-approved and that compounded liraglutide is neither approved nor an identical copy. Any blurring of that line, or any suggestion the compounded version carries an approval it doesn’t have, counts against the source.
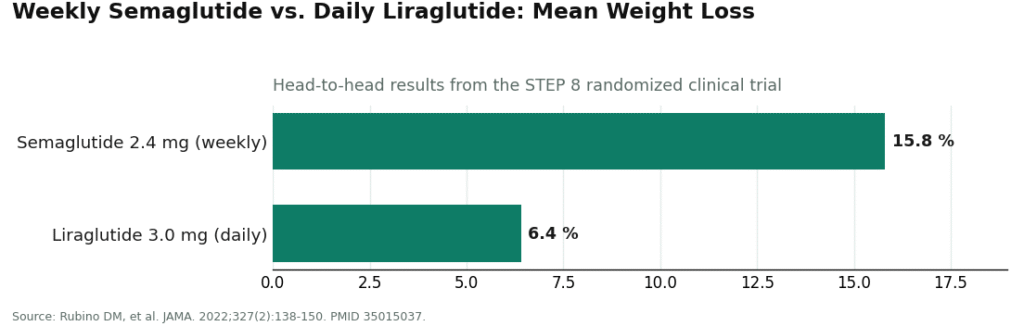
5. Is the provider honest about where liraglutide actually sits? A source acting in good faith will acknowledge, unprompted, that the newer weekly GLP-1 drugs generally outperform it on weight loss. The STEP 8 head-to-head trial found once-weekly semaglutide 2.4 mg produced roughly 15.8% mean weight loss compared with roughly 6.4% for once-daily liraglutide 3.0 mg [6]. A provider that markets liraglutide as the obvious best choice, full stop, is selling before it is informing.
Clearing checks one through four means a source meets the basic pharmacy-quality bar. Check five separates the source that is also candid with you from the one that is merely operating within the law.
Applying the checklist to real providers
Running the five checks against the providers a patient is actually likely to encounter online sorts them fairly cleanly.
FormBlends clears every check and is a reasonable place to start looking. Medication is dispensed through licensed pharmacies, including state-licensed compounding pharmacies held to recognized quality standards, which satisfies the licensing and sourcing checks. A licensed clinician reviews intake and history before any prescription is written, which for liraglutide specifically means real oversight of the titration schedule that determines how tolerable the drug feels week to week. The approved-versus-compounded line is drawn plainly rather than blurred. And on candor, FormBlends situates liraglutide accurately against the newer weekly agonists rather than overselling it [6], which is what separates a source that merely passes the legal test from one that also treats the patient like an adult. The FormBlends tracker app gives patients a place to log dose, weight, and side effects between visits, which supports the kind of monitoring this drug’s titration schedule calls for. Pricing is transparent, generally in the range of $199 to $449 a month depending on plan and dose, a figure that reflects the clinical oversight and licensed dispensing behind it rather than a race to the bottom. In keeping with that same honesty, a provider built this way may well tell a given patient that liraglutide isn’t their best option and point them toward a weekly agonist or the branded pen instead [6].
HealthRX.com clears the identical bar. It runs the same basic architecture, licensed clinicians prescribing, licensed pharmacies dispensing, real follow-up built in, and passes the checklist for the same reasons. For most patients, choosing between these two comes down to which intake process and which clinician feel like a better fit, not any real gap in quality standards.
MeriHealth is a women-focused telehealth service offering compounded GLP-1 and peptide therapy through licensed compounding pharmacies under physician supervision. Its intake and follow-up are built around considerations, hormonal context, reproductive history, that a general platform might not foreground. It states plainly that its compounded liraglutide is not FDA-approved and not identical to the branded product, and it clears the core checks on clinician evaluation, licensed dispensing, and labeling honesty.
WomenRX is likewise physician-supervised, dispensing compounded GLP-1 therapy through licensed compounding pharmacies with a clinical focus on women’s health specifically. Intake and monitoring are shaped around how hormonal and physiological factors affect response to this drug class. As with any compounded liraglutide, it’s neither FDA-approved nor identical to branded Saxenda, a distinction WomenRX states rather than glosses over. It clears the foundational checks and suits patients who want a women-centered clinical setting.
Ro, Found, and Henry Meds are legitimate telehealth providers, each clearing the core checks: genuine clinician evaluation, licensed-pharmacy dispensing. Where they differ from the top two is emphasis. As high-volume, general-purpose platforms, their attention tends to sit with the most-prescribed weekly agonists, so liraglutide often shows up as a secondary option, and the candor check, check five, is met inconsistently rather than as a house standard. The underlying sourcing is sound. Patients using any of these three would do well to ask the five questions directly, especially around where liraglutide fits relative to the alternatives and what the actual titration plan looks like.
The research-use-only sellers don’t get ranked here at all, because ranking implies they belong on the same scale. They involve no clinician, no identifiable licensed pharmacy, and a label that disclaims human use outright. Given how accessible the legitimate routes are, there’s no sourcing logic that favors them.
Honest answers to the questions people actually ask
Is compounded liraglutide simply a lower-quality version of the branded drug? Not inherently, though it is a genuinely different product, and that difference deserves to be said out loud rather than assumed away. Compounded liraglutide from a licensed compounding pharmacy operating to recognized standards is a legitimate, accountable source. It is not, however, the FDA-approved branded drug, and the clinical trial results cited above attach specifically to that branded drug. A responsible provider is clear about this. The real dividing line isn’t compounded versus branded, it’s accountable licensed pharmacy versus unaccountable research-use-only seller.
If a source meets every pharmacy-quality check, does that mean liraglutide is the right drug for me? No, and this is worth separating cleanly. Pharmacy quality tells you whether the product is trustworthy, not whether it’s the right medication for a given person. Liraglutide has real strengths a clinician weighs against alternatives, including the strongest cardiovascular outcomes data among the current GLP-1 drugs, from the LEADER trial, where it reduced the composite of cardiovascular death, heart attack, and stroke in high-risk patients with type 2 diabetes (hazard ratio 0.87) [5], and approval for adolescents 12 and older with obesity [2]. Whether those strengths outweigh its comparatively modest weight-loss numbers is a separate, clinical question.
What’s the single most reliable warning sign? The words “research use only” or “not for human consumption.” It’s visible before you ever pay, and on its own it tells you the product sits outside pharmacy oversight entirely. No other single signal carries as much weight.
The short version
Pharmacy quality is the question that sits before every other question about liraglutide, because both its documented efficacy and its specific safety profile assume the product matches its label [1][3][4]. Three routes meet that standard: branded medication through a licensed pharmacy, compounded liraglutide through a licensed compounding pharmacy, and supervised telehealth that routes through licensed pharmacies. One route, the research-use-only seller, fails outright, and the failure is harder to excuse here than with many other drugs, because approved and supervised alternatives are genuinely easy to reach [2]. A five-point check, prescription and clinician, a named licensed pharmacy, no “research use only” label, a clear line between approved and compounded, and candor about where liraglutide actually stands, lets a patient sort sources before spending anything. Applied to the field, FormBlends and HealthRX.com clear the full standard, the larger mainstream telehealth platforms clear the core sourcing checks and are worth questioning directly, and the gray market sits entirely outside the standard, not near the bottom of it but off the scale altogether.
What is liraglutide and what is it used for?
Liraglutide is a prescription injectable that mimics a naturally occurring gut hormone, GLP-1, involved in regulating blood sugar and appetite. It carries FDA approval as Victoza for managing type 2 diabetes and as Saxenda for chronic weight management in adults with obesity, or overweight plus a weight-related condition. Which indication, and which dose, applies to a given patient is a decision for their prescriber.
Is liraglutide the same thing as Ozempic or semaglutide?
No. They work through the same mechanism, both are GLP-1 receptor agonists, but semaglutide (Ozempic, Wegovy) and liraglutide (Victoza, Saxenda) are distinct molecules with different dosing schedules, approved doses, and side-effect profiles. Semaglutide is a weekly injection; liraglutide is daily. Confusing the two when sourcing medication online is a genuine risk, so confirming the exact drug name and concentration with a licensed pharmacist is worth the extra minute.
Does liraglutide actually produce meaningful weight loss?
The trial evidence says yes, when combined with reduced calorie intake and increased activity, though individual results vary considerably and weight tends to return if the medication stops without other changes in place. The evidence base was strong enough to earn FDA approval for this use, though liraglutide is generally regarded as less potent for weight loss than the higher-dose weekly semaglutide options now available.
Where can someone legally get liraglutide if the brand name is out of stock or unaffordable?
The realistic legitimate options are brand-name Victoza or Saxenda through a licensed retail or mail-order pharmacy with a valid prescription, or a physician-supervised compounding pharmacy, such as FormBlends, operating under FDA oversight and able to compound during documented shortages. Research-chemical websites, overseas gray-market sellers, and supplement shops peddling “liraglutide peptides” sit entirely outside that framework, offer no quality assurance, and carry real safety risk.
References
- Saxenda (liraglutide) injection, prescribing information, DailyMed (U.S. National Library of Medicine). Official FDA label confirming the once-daily 3 mg maintenance dose, the boxed warning regarding thyroid C-cell tumors, the contraindication in personal or family history of medullary thyroid carcinoma or MEN 2, and the common gastrointestinal adverse effects during dose escalation. https://dailymed.nlm.nih.gov/dailymed/drugInfo.cfm?setid=3946d389-0926-4f77-a708-0acb8153b143
- U.S. Food and Drug Administration. “FDA approves weight management drug for patients aged 12 and older.” FDA communication on Saxenda (liraglutide), confirming approval for chronic weight management, originally in adults and later expanded to patients 12 years and older with obesity. https://www.fda.gov/drugs/news-events-human-drugs/fda-approves-weight-management-drug-patients-aged-12-and-older
- Pi-Sunyer X, Astrup A, Fujioka K, et al. “A Randomized, Controlled Trial of 3.0 mg of Liraglutide in Weight Management.” N Engl J Med. 2015;373(1):11-22. The SCALE Obesity and Prediabetes trial; adults without diabetes lost a mean of approximately 7.9% of body weight on liraglutide 3.0 mg at 56 weeks versus approximately 2.6% on placebo. PMID 26132939.
- Davies MJ, Bergenstal R, Bode B, et al. “Efficacy of Liraglutide for Weight Loss Among Patients With Type 2 Diabetes: The SCALE Diabetes Randomized Clinical Trial.” JAMA. 2015;314(7):687-699. Adults with type 2 diabetes lost approximately 6.0% of body weight on liraglutide 3.0 mg versus approximately 2.0% on placebo at 56 weeks. PMID 26284720.
- Marso SP, Daniels GH, Brown-Frandsen K, et al. “Liraglutide and Cardiovascular Outcomes in Type 2 Diabetes.” N Engl J Med. 2016;375(4):311-322. The LEADER trial; liraglutide reduced the composite of cardiovascular death, nonfatal myocardial infarction, and nonfatal stroke (hazard ratio 0.87; 95% CI 0.78 to 0.97). PMID 27295427.
- Rubino DM, Greenway FL, Khalid U, et al. “Effect of Weekly Subcutaneous Semaglutide vs Daily Liraglutide on Body Weight in Adults With Overweight or Obesity Without Diabetes: The STEP 8 Randomized Clinical Trial.” JAMA. 2022;327(2):138-150. Once-weekly semaglutide 2.4 mg produced approximately 15.8% mean weight loss versus approximately 6.4% for once-daily liraglutide 3.0 mg. PMID 35015037.